 2015, Vol. 35
2015, Vol. 35

2. 兰州大学附属第一临床医学院研究生院


放射治疗是乳腺癌患者术后的重要辅助治疗之一,可以改善患者的局部控制率及总生存率。几个大型前瞻性多中心临床研究及早期乳腺研究协作组(EBCTCG)的最新研究结果均显示,对于乳腺癌术后腋窝淋巴结转移≥4个,以及原发肿瘤T3及以上的局部(包括区域淋巴结)复发高危患者术后放疗可明显获益[1, 2, 3]。美国国家综合癌症网络(NCCN)指南也支持这一观点[4]。而对于术后1~3个腋淋巴结转移的T1、T2期乳腺癌患者,是否放疗争议很大[5, 6]。本研究采用Cochrane系统评价方法,探讨乳腺癌患者(改良)根治术后腋淋巴结转移1~3个的T1或T2患者行术后放疗的疗效,结合临床收集证据,为进一步治疗提供可靠的依据。
1.资料来源:检索数据库包括:PubMed数据库、EMBASE数据库、Web of science数据库、中国期刊全文数据库、中国生物医学文献数据库、中国科技期刊数据库和万方全文数据库。末次检索时间为2014年12月31日。
2. 检索方法:本研究采用电子检索和文献追溯检索。英文检索主题词有breast neoplasm、positive lymph nodes、radiotherapy,中文检索主题词包括:乳腺癌、腋窝淋巴结、放射治疗,并追查已纳入文献的参考文献。所有检索均采用自由词与主题词[MEDLINE (MeSH),EMBASE (EMTREE)]相结合的方式,反复检索之后确定最终检索方法。
3. 纳入与剔除标准:纳入标准包括:临床对照研究,文种限中文及英文;研究对象为经病理组织学证实为乳腺癌患者,按照(AJCC)或(UICC)分期标准[7],所有纳入的病例均为T1、T2(直径≤5 cm)及腋窝淋巴结转移1~3个行(改良)根治术的患者;没有伴发其他肿瘤;无远处转移及其他并发症。干预措施:试验组为术后行放疗患者,放疗区域至少包括胸壁;对照组为术后未放疗患者。剔除标准:腋窝淋巴结清扫不彻底(中位数<10个);行保乳手术;术前行化疗或放疗;随访时间<5年的患者。
4. 文献筛选及资料提取:筛选过程中由2名研究人员独立按照纳入和排除标准严格筛选文献,提取资料。如遇分歧,讨论解决,必要时征询第三方意见以达成一致。
5. 统计学处理:采用RevMan 5.2软件进行Meta分析,计数资料以比值比(OR)作为合并分析的统计量,并计算其95%的可信区间(95% CI)。统计学差异性检验首先采取Q检验和I2统计量,Q检验中若P≥0.1且I2<50%,提示研究间同质性好,采用固定效应模型分析;若P<0.1且I2>50%,则研究结果间同质性差,可分析其异质性的来源,对可能导致异质性的因素进行亚组分析。若各个研究间存在统计学异质性而无临床异质性,则采用随机效应模型分析,并谨慎解释结果。P<0.05认为结果可信,反之不可信。
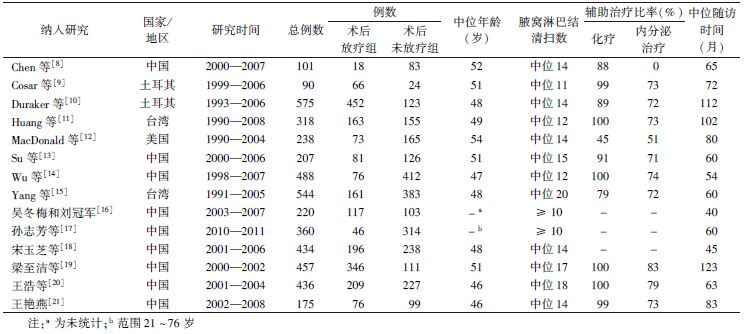
1. 检索结果:初检相关文献425篇(英文305篇,中文120篇),通过阅读题目及摘要,排除综述类文献、信件、重复发表、动物实验及明显不符合纳入标准的文献401篇,剩余23篇阅读全文,严格按照纳入及排除标准筛选,其中数据不全且无法补充文献3篇,无对照组文献3篇,综述类文献2篇,重复报道文献1篇,最终纳入文献共14篇(英文8篇,中文6篇)[8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21];共4 643例患者,其中,放疗组2 080例,未放疗组2 563例患者。所有研究靶区均包括胸壁并行常规分割,吸收剂量为45~55 Gy。文献纳入研究的基本特征列于表1。
| 表1 乳腺癌(改良)根治术后1~3个腋淋巴结阳性的T1~T2期患者Mata分析纳入研究的基本资料 |
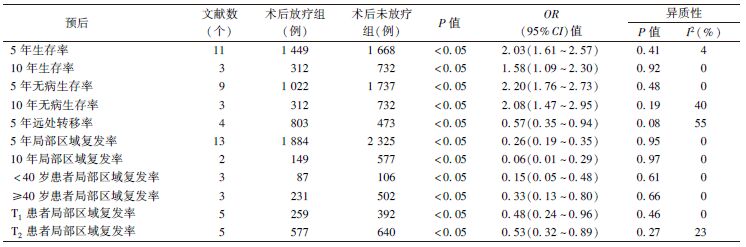
2. Meta分析结果:11个研究报道了5年生存率[9, 11, 12, 13, 14, 16, 17, 18, 19, 20, 21],3个研究报道了10年生存率[11, 12, 14],Meta分析结果显示,与术后未放疗组相比,术后放疗组的5年生存率(OR 2.03,95% CI 1.61~2.57,P<0.05)及10年生存率(OR 1.58,95% CI 1.09~2.30,P<0.05)均明显提高。9个研究报道了5年无病生存率[9, 11, 12, 14, 16, 17, 18, 20, 21],3个研究报道了10年无病生存率[11, 12, 14],与术后未放疗组相比,术后放疗组的5年无病生存率(OR 2.20,95% CI 1.76~2.73,P<0.05)及10年无病生存率(OR 2.08,95% CI 1.47~2.95,P<0.05)均有明显提高。4个研究报道了5年远处转移率[9, 10, 20, 21],结果显示,术后放疗组与术后未放疗组相比,术后放疗组的5年远处转移率(OR 0.57,95% CI 0.35~0.94,P<0.05)明显下降。13个研究报道了5年局部区域复发率[8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 19, 20, 21],2个研究报道了10年局部区域复发率[12, 14],与术后未放疗组相比,术后放疗组的5年局部区域复发率(OR 0.26,95% CI 0.19~0.35,P<0.05)及10年局部区域复发率(OR 0.06,95% CI 0.01~0.29,P<0.05)均明显降低。分别按照年龄(<40岁和≥40岁)及肿瘤的大小(T1直径≤2 cm和2 cm<T2直径 ≥5 cm)进行亚组分析,结果显示,与术后未放疗组相比,术后放疗组中<40岁患者及≥40岁患者的局部区域复发率均明显降低,T1患者局部区域复发率及T2患者局部区域复发率术后放疗组比术后未放疗组明显下降,详细结果列于表2。
| 表2 术后放疗组对比术后未放疗组的14个研究Meta分析结果 |
3. 发表偏倚:漏斗图结果如图1所示,显示纳入研究分布不对称,有发表偏倚的可能性。发表偏倚是指由于研究者、审者及编辑在选择论文发表时依赖研究结果的方向与强度所产生的偏差,即具有阳性结果的研究比阴性结果的研究更容易发表。

|
图1 术后放疗对局部区域复发率的漏斗图 |
本研究结果表明,术后放疗对T1、T2腋窝淋巴结转移1~3个的患者有明显的疗效。欧洲癌症治疗研究组织(EORTC)一项回顾性研究分析了3项大的研究中共3 648例患者的病例资料,结果显示,乳腺癌术后放疗不仅可以降低局部区域复发率,还能改善生存率;而获益最明显的是腋窝淋巴结1~3个阳性的患者[22]。在丹麦的一项随机研究亚组分析中显示,术后放疗对该群患者有生存获益[23]。随后,该研究更新报道了仅分析腋窝淋巴结检出数≥8个、腋窝淋巴结转移1~3个的患者,发现放疗可将局部区域复发率从27%降到4%,并提高了15年的总生存率,由48%增加到57%,而且,1~3个腋淋巴结阳性患者接受放疗获益的幅度高于4个以上淋巴结阳性患者[24]。
乳腺癌是一类分子水平上具有高度异质性的疾病。多项研究显示,年龄、T分期、淋巴结阳性个数、淋巴、血管受侵和激素受体表达等是影响局部控制率的预后因素。本研究Meta分析分别对年龄(≥40和<40岁)及肿瘤的大小(T1直径≤2 cm和2 cm<T2直径≤5 cm)进行亚组分析,结果显示,无论年龄及肿瘤大小,术后放疗的局部区域复发率均明显下降,但两组对于生存率的影响还有待进一步研究。根据早期乳腺癌国际协作组荟萃分析的结果,每降低4个局部或区域复发,可避免1例死亡,总生存率的提高同局部或区域复发率降低相关[25]。年龄作为独立的预后因素,各项研究对此的报道并不一致。有研究报道,年轻患者由于肿瘤分级高、血管受侵多级、ER阴性比率更高等原因其预后较差[26]。Tai等[27]认为,年龄和乳腺癌死亡之间存在双相关系,类似U型函数,即年轻患者和年老患者的预后均较差。另外,淋巴结清扫不彻底可能会导致腋窝有转移淋巴结残留,低估腋窝淋巴结的转移程度,从而使这部分患者复发率相对较高、长期生存率下降。本研究纳入的病例均为腋窝淋巴结清除中位数≥10个,相对降低了对结果的影响,提高了结果的可信性。淋巴结外浸润和组织学Ⅲ级也是T1、T2期伴1~3个阳性淋巴结乳腺癌患者预后的危险因素,放疗可以明显改善有这些危险因素患者的局部复发和总生存率[19, 28]。肿瘤大小和受体状态等因素亦是该类患者预后的危险因素[29, 30]。
化疗及内分泌治疗对结果的影响也不容忽视。本研究中仅有3个研究未统计化疗及内分泌治疗的人数,其余研究中纳入的患者都行术后辅助性的治疗。EBCTCG的Meta分析显示,术后辅助化疗及内分泌对比单纯术后其局部区域复发率明显下降,并且有明显的生存获益[3]。因此,纳入的患者获益有一部分来源于化疗及内分泌治疗。对于术后腋窝淋巴结1~3个转移患者放疗靶区的确定,目前尚无定论。2014版NCCN指南中指出,对于全乳切除术+外科腋窝分期(1类)±乳房重建患者中1~3个阳性腋窝淋巴结者,强烈建议化疗后行胸壁及锁骨上、下区域放疗;如果要进行放疗,应考虑内乳淋巴结放疗(2B类)[4]。
对于根治术后腋窝淋巴结1~3个阳性的患者,本研究结果进一步肯定了放疗对其降低局部区域复发率、提高总生存率的疗效,为术后T1、T2期腋窝淋巴结1~3个转移患者选择放疗提供参考。但上述结论仍需要随机双盲对照试验加以证实。目前,正在进行的欧洲癌症与研究治疗组的前瞻性临床随机试验,其入组对象包括T1~T2期1~3枚淋巴结转移患者,入组患者随机进入胸壁放疗组或未放疗组,但目前还未完成[31]。期待今后的临床随机试验可以提供合适的放疗方案,以应用于合适的患者。
| [1] | Overgaard M, Jensen MB, Overgaard J, et al. Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial[J]. Lancet, 1999, 353(9165): 1641-1648. |
| [2] | Ragaz J, Olivotto IA, Spinelli JJ, et al. Locoregional radiation therapy in patients with high-risk breast cancer receiving adjuvant chemotherapy: 20-year results of the British Columbia randomized trial[J]. J Natl Cancer Inst, 2005, 97(2): 116-126. |
| [3] | Early Breast Cancer Trialists' Collaborative Group. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8 135 women in 22 randomised trials[J]. Lancet, 2014, 383(9935): 2127-2135. |
| [4] | National Comprehensive Cancer Network. 2014 NCCN Breast Cancer Guidelines (Version 3.2014)[R]. America: NCCN, 2014. |
| [5] | Marks LB, Zeng J, Prosnitz LR. One to three versus four or more positive nodes and postmastectomy radiotherapy: time to end the debate[J]. J Clin Oncol, 2008, 26(13): 2075-2077. |
| [6] | Voordeckers M, Vinh-Hung V, Lamote J, et al. Survival benefit with radiation therapy in node-Positive breast carcinoma patients[J]. Strahlenther Onkol, 2009,185(10): 656-662. |
| [7] | Singletary SE, Connolly JL. Breast cancer staging: working with the sixth edition of the AJCC cancer staging manual[J]. CA Cancer J Clin, 2006, 56(1): 37-47. |
| [8] | Chen X, Yu X, Chen J, et al. Radiotherapy can improve the disease-free survival rate in triple-negative breast cancer patients with T1-T2 disease and one to three positive lymph nodes after mastectomy[J]. Oncologist, 2013, 18(2): 141-147. |
| [9] | Cosar R, Uzal C, Tokatli F, et al. Postmastectomy irradiation in breast cancer patients with T1-2 and 1-3 positive axillary lymph nodes: is there a role for radiation therapy?[J]. Radiat Oncol, 2013, 6:28. |
| [10] | Duraker N, Demir D, Bati B, et al. Survival benefit of post-mastectomy radiotherapy in breast carcinoma patients with T1-2 tumor and 1-3 axillary lymph node(s) metastasis[J]. Jpn J Clin Oncol, 2012, 42(7):601-608. |
| [11] | Huang CJ, Hou MF, Chuang HY, et al. Comparison of clinical outcome of breast cancer patients with T1-2 tumor and one to three positive nodes with or without postmastectomy radiation therapy[J]. Jpn J Clin Oncol, 2012, 42(8): 711-720. |
| [12] | MacDonald SM, Abi-Raad RF, Alm El-Din MA, et al. Chest wall radiotherapy: middle ground for treatment of patients with one to three positive lymph nodes after mastectomy[J]. Int J Radiat Oncol Biol Phys, 2009, 75(5): 1297-1303. |
| [13] | Su YL, Li SH, Chen YY, et al. Post-mastectomy radiotherapy benefits subgroups of breast cancer patients with T1-2 tumor and 1-3 axillary lymph node(s) metastasis[J]. Radiol Oncol, 2014, 48(3): 314-322. |
| [14] | Wu SG, He ZY, Li FY, et al. The clinical value of adjuvant radiotherapy in patients with early stage breast cancer with 1 to 3 positive lymph nodes after mastectomy[J]. Chin J Cancer, 2010, 29 (7):668-676. |
| [15] | Yang PS, Chen CM, Liu MC, et al. Radiotherapy can decrease locoregional recurrence and increase survival in mastectomy patients with T1 to T2 breast cancer and one to three positive nodes with negative estrogen receptor and positive lymphovascular invasion status[J]. Int J Radiat Oncol Biol Phys, 2010, 77(2): 516-522. |
| [16] | 吴冬梅,刘冠军. 术后放疗对早期伴有1-3个阳性淋巴结乳腺癌患者的临床价值及其预后因素分析[J].实用医学杂志, 2013, 29(2): 230-232. |
| [17] | 孙志芳,胡延良,王季秋,等. T1-T2 期腋窝淋巴结1-3 个转移乳腺癌改良根治术后放疗的疗效及影响因素[J]. 现代预防医学, 2012, 39(22):5846-5848. |
| [18] | 宋玉芝,耿翠芝,乔学英. 1-3个腋淋巴结阳性的T1-T2期乳腺癌改良根治术后患者预后因素分析[J]. 肿瘤, 2011, 31(8):735-741. |
| [19] | 梁至洁,贾苗苗,陈钦,等. 术后放疗对T1-2 期伴1-3 枚淋巴结转移乳腺癌患者预后的影响[J].中国肿瘤临床, 2014, 41(8):498-502. |
| [20] | 王浩,罗杨坤,王捷,等. 放疗对改良根治术后T1-T2 期伴1-3个腋窝淋巴结转移乳腺癌不同分子亚型患者预后影响[J]. 中华放射肿瘤学杂志, 2011, 20(5): 397-401. |
| [21] | 王艳燕. 1-3个淋巴结转移的早期乳腺癌局部复发因素在确定术后放疗指证中的应用价值[D]. 长沙:中南大学,2013. |
| [22] | van der Hage JA, Putter H, Bonnema J, et al. Impact of locoregional treatment on the early-stage breast cancer patients: a retrospective analysis[J]. Eur J Cancer, 2003, 39(15): 2192-2199. |
| [23] | Overgaard M, Hansen PS, Overgaard J, et al. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. Danish Breast Cancer Cooperative Group 82b Trial[J]. N Engl J Med, 1997, 337(14): 949-955. |
| [24] | Overgaard M, Nielsen HM, Overgaard J, et al. Is the benefit of postmastectomy irradiation limited to patients with four or more positive nodes, as recommended in international consensus reports? A subgroup analysis of the DBCG 82 b&c randomized trials[J]. Radiother Oncol, 2007, 82(3): 247-253. |
| [25] | Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year surival:an overview of the randomised trials[J]. Lancet, 2005, 366(9503): 2087-2106. |
| [26] | Han W, Kim SW, Park IA, et al. Young age:an independent risk factor for disease-free survival in women with operable breast cancer?[J]. BMC Cancer, 2004, 4: 82. |
| [27] | Tai P, Cserni G, van De Steene J, et al. Modeling the effect of age in T1-2 breast cancer using the SEER database[J]. BMC Cancer, 2005, 5: 130. |
| [28] | Moo TA, McMillan R, Lee M, et al. Selection criteria f or postmastectomy radiotherapy in T1-T2 tumors with 1 to 3 positive lymph nodes[J]. Ann Surg Oncol, 2013, 20(10): 3169-3174. |
| [29] | Tendulkar RD, Rehman S, Shukla ME, et al. Impact of postmastectomy radiation on locoregional recurrence in breast cancer patients with 1-3 positive lymph nodes treated with modern systemic therapy[J]. Int J Radiat Oncol Biol Phys, 2012, 83(5): e577-581. |
| [30] | Katz A, Strom EA, Buchholz TA, et al. Locoregional recurrence patterns after mastectomy and doxorubicin-based chemotherapy: implications for postoperative irradiation[J]. J Clin Oncol, 2000,18(15): 2817-2827. |
| [31] | Kunkler IH, Canney P, van Tienhoven G, et al. Elucidating the role of chest wall irradiation in 'intermediate-risk' breast cancer: the MRC/EORTC SUPREMO trial[J]. Clin Oncol, 2008, 20(1): 31-34. |