 2015, Vol. 35
2015, Vol. 35



2. Peking Union Medical College Hospital
Helical tomotherapy unit (TOMO unit) is a kind of equipment integrated with CT and linear accelerator together,specifically designed for image-guided intensity modulated radiation therapy (IMRT). The image-guided IMRT with TOMO unit is implemented by using megavoltage CT (MVCT) in real-time while continuous rotation and couch moving are actualized in a mode which similar to a spiral CT scanning,and it represents the tomo-radiotherapy technology in the latest generation[1, 2, 3, 4]. Because fan-shaped narrow beam treatment style and online MVCT are used simultaneously,not only the position change of patient focus should be monitored in the course of treatment,but also the irradiation dose delivered to patient every time should be rebuilt through the acquisition of online 3D images,and the excess dose area and deficient dose area can be determined by comparing with the iso-dose curve of original treatment plan. Therefore,an individual dose guided adaptive radiotherapy (dose guided adaptive radiation therapy,DGART) can be achieved under the guidance of subsequent adjustment for radiotherapy dose of the interest region.
The quality control (QC) is important particularly because of the characteristics of TOMO unit including both high IMRT dose conformal rate of TOMO dose distribution and quick fall outside the target area dose in the massive focusing irradiation[5]. Therefore,a series of related performance parameters and test requirements are presented according to the technical report of AAPM No.148[6]. At present,the clinical TOMO units are belonged to the series of Hi-Art TomoTherapy which were developed by the American tomotherapy company. Since the first TOMO unit was employed in clinic in 2003,there are more than 500 U in the world and more than 10 sets of TOMO units in our country. In the study,the test and analyses on dosimetric and radiation safety performance parameters of the Hi-Art tomotherapy were executed to understand the functional status and radiation protection requirements of the unit when it was applied in clinic treatment so as to promote the construction of TOMO quality control system.
A TOMO unit with a type of tomotherapy Hi-Art was employed as the radiation treatment equipment. The main parameters of the unit were as follows. The maximum electron energy of accelerator was 6 MV. Source axis distance (SAD) was 85 cm. The maximum dose rate at isocenter was 10 Gy/min (equivalent to 600 Gy/h) and the mean value was 8.8 Gy/min (or 528 Gy/h). The beam stopper opposite primary beam was 13 cm lead. The treatment beam was fan-shaped narrow beam,and the maximum radiation field size at the isocenter was 5 cm×40 cm (5 cm of the maximum beam opening or thickness,40 cm of the maximum beam width). The treatment unit also had a 3.5 MV CT image device with low radiation output dose of X-ray,and the absorbed dose received by a patient was only 1-3 cGy when the MVCT scanned in each treatment scan. In the study,the performance parameters test results of TOMO unit were compared with that of a conventional 6 MV accelerator with a type of ARTISTE.
2. Test instruments and toolsThe test instruments and tools used in the study including an A1SL ionization chamber (0.056 cm3,Standard Imaging,USA),a tomoelectrometer dosimeter (Standard Imaging,USA),a set of rectangular solid water phantom (Med-Cal,USA) with a size of 15 cm×55 cm,a cylindrical solid water phantom (Med-Cal,USA) with multiple ionization chamber hole and inserting rod of different density,a TOMO water tank,TOMODOSE verification system,over 300 thermoluminescent dosimeters (TLDs).
3. The parameters to be measured and test methodsStatic output dose: TOMO accelerator head was set to 0 degree,and the radiation field size was adjusted to 40 cm×5 cm,40 cm×2.5 cm and 40 cm×1 cm with the same SSD(85 cm) respectively. The second step was that the A1SL ionization chamber was positioned under 1.5 cm from the surface of rectangular solid water phantom. The tomoelectrometer instrument was connected with A1SL ionization chamber with +300 V bias before measurement of charge sampling start. The collective time was 70 s.
Dynamic output dose (IMRT planning dose or a rotary output dose): The A1SL ionization chamber was irradiated when TOMO accelerator performs a clinical treatment plan.
Radiation quality: After the A1SL ionization chamber was placed in the rectangular solid water phantom,the output dose at the three positions including 1.5,10 and 20 cm under the surface of the phantom could be tested under the condition of the same measuring time,and the two ratios of PDD10 / PDD1.5 and PDD20 / PDD1.5 would be calculated from PDD1.5,PDD10 and PDD20 before they were evaluated on the basis of the reference ratio in the acceptance test.
Stability of horizontal/vertical dose distribution curves: The acceptance testing of the dose distribution was tested by TOMO water tank scanning system after the target of TOMO treatment unit has been changed. The x and y axis dose distribution curves in three different sizes of static field of 40 cm × 5 cm,40 cm × 2.5 cm and 40 cm × 1 cm were obtained under the different scanning depths of 1.5,5,10,15 and 20 cm. At the same time,the dose distribution curve of x and y axis at 1.5 cm depth were measured and verified by TOMODOSE verification system,and they were compared with dose distribution curves from water tank scanning. Also,its stability was checked through the dose distribution curve.
The offset distance of Jaw width: By means of the measurement method shown in step (Stability of horizontal/vertical dose distribution curres),the y value could be displayed directly from the analytical results in the longitudinal dose distribution curve,and compared with y (cm) preset.
Leakage radiation dose level from multileaf collimator: The rectangular phantom was connected with the dosimeter as step (Static output dose),and the width of second collimation was set to 5 cm. The next step was that the irradiation of same integrated time was operated under the full closed state and full open state of multileaf collimator respectively,the dosimeter readings of the two kinds of conditions were recorded and the reading ratios were calculated respectively.
The leakage radiation levels of TOMO treatment room: Thermoluminescence dosimeter (TLD) was used in the parameter measurement,and the TLD detection elements LiF (Mg,Cu,P) thermoluminescence detector with a type of GR-200A,which was wafer disc with φ4.5 mm×0.8 mm. Before the dose level of radiation from the leakage in the treatment couch plane was measured,the TLDs must be put on the circles with radius of 100,200 and 300 cm around the circumvolve isocenter of TOMO facility in the couch plane respectively (Figure 1),and the cumulative beam from simulate circumvolve radiotherapy in 20 s/circle was set to 100 Gy under the condition of all collimators close and open seperately. Therefore,the leakage radiation ratios could be calculated by comparing with the TLD dose and output dose preset.
 | Figure 1 Measuring point settings for leakage radiation in the TOMO treatment couch plane |
The dose output parameters of TOMO unit consisted of static and dynamic output dose,and the deviation between the measured and preset dose could be calculated by means of the above measuring method. Under the conditions of different static fields of 40 cm×5 cm,40 cm×2.5 cm and 40 cm×1 cm,the output dose rate of the TOMO unit were 854.39,829.62 and 664.98 cGy/min,respectively. The error for the static field of 40 cm×5 cm was -1.51% compared to 867.50 cGy/min which was the first testing result after the target of TOMO unit had been changed last time. At the same time,under the condition of the static output,the repeatability error of the corresponding dose output was 0.07% calculated from the readout values of five times. At the same way,all dose output error and coefficient variation of the other static field sizes (40 cm×2.5 cm and 40 cm×1 cm) were less than 2.00% and 0.70%,respectively.
A planned dose file called "DQA TRMT-Completion" was chosen from treatment planning system to verify the dynamic output dose. Under the typical treatment irradiation conditions of the target area of 14 cm to y direction,2 Gy of single irradiation dose,2.5 of modulation factor,20 s per rotating cycle and 0.43 of pitch ratio,the measured output dose integrated of 361 s was 196.10 cGy,and the error between the measured dose and the planned dose (193.80 cGy) was 1.18%. The test results showed that the parameters of static output dose and dynamic output dose met the requirements of AAPM TG-148 and equipment manufactory which was no more than 2.00%. In general,the error between prescription treatment dose and measured dose should be less than 3.00% according to GBZ 126-2011 for conventional electron accelerator,and the parameter of TOMO unit was stricter than that of conventional electron linear accelerator because of its special treatment features.
2. Treatment radiation quality and dose distributionRadiation quality value was derived from the comprehensive analysis of PDD1.5,PDD10 and PDD20. At first,the value of PDD10 / PDD1.5 and PDD20 / PDD1.5 were confirmed on the basis of the radiation quality values measured and the steady state of TOMO unit,then the single measure results could be identified whether they were in the calibration range or not. In this study,PDD10/PDD1.5 of 0.608 and PDD20/PDD1.5 of 0.318 were all within the scope of the calibration,because the radiation energy calibration parameters of the TOMO unit were in the range of 0.596-0.623 and 0.315-0.328,respectively.
Dose distribution parameters included the stability of vertical and horizontal dose distribution curves as well as the offset distance of Jaw width. The dose distribution curves of the x and y axes were obtained by TOMO tank scanning under the conditions of different fields and different depths previously. The different adjusted fields included 40 cm × 5 cm,40 cm × 2.5 cm and 40 cm ×1 cm,and different scanning depths including 1.5,5.0,10,15 and 20 cm distance away from the water phantom surface respectively. The dose distribution curves of the 40 cm × 2.5 cm at different depths were shown in Figure 2 and 3. The dose distribution curve for 1.5 cm depth was also verified by using TOMODOSE verification system and the results were shown in table 1.
 | Figure 2 Dose distribution curve of 40 cm× 2.5 cm static radiation field at the x axis of TOMO unit |
 | Figure 3 Dose distribution curve of 40 cm× 2.5 cm static radiation field at the y axis of TOMO unit |
| Table 1 Verification results of stability of dose distribution curve and error of Jaw width for TOMO unit |
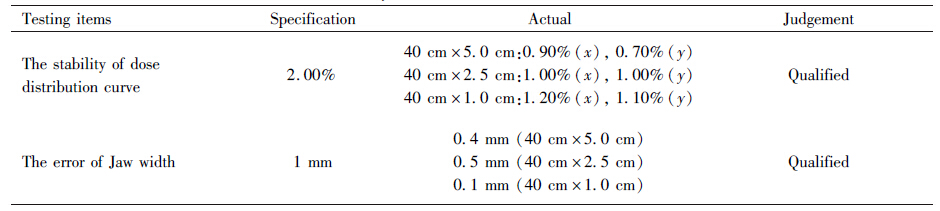
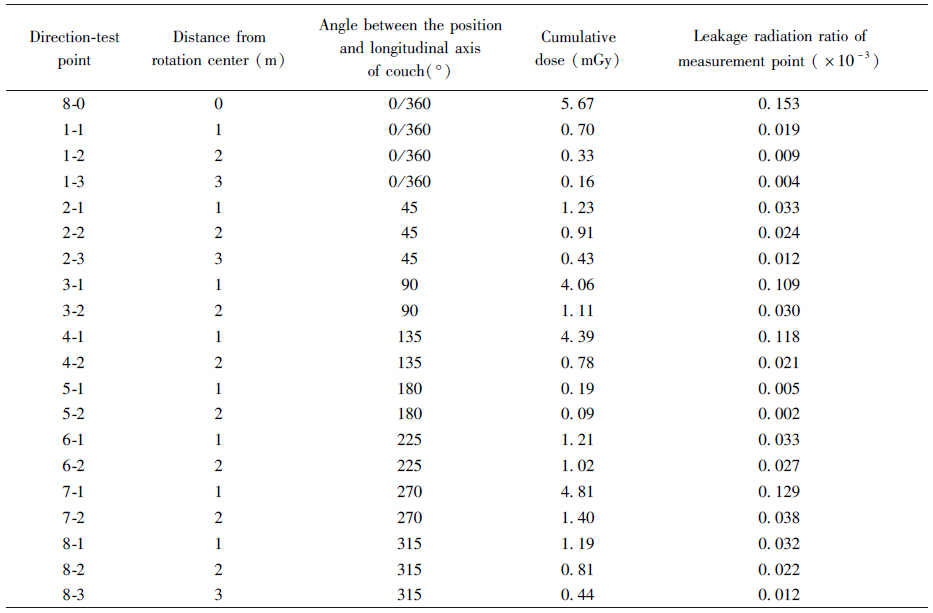
The leakage radiation parameters of TOMO unit included the leakage radiation levels of multileaf collimator and treatment couch plane,and they were representative of core radiological protection performance. Under the conditions of multileaf collimator closed state and open state separately while second collimator open with width of 5 cm,the charge readings displayed on the dosimeter were 0.03 and 14.11 in 60 s of beam-on time,respectively. The leakage radiation ratio of multileaf at rotation center was 0.20%. In the leakage radiation test of treatment couch plane,TLDs were irradiated for 3 716 cGy after measurement point setting project being finished as above,and the TLD measurement results were shown in table 2. The average and maximum values of radiation leakage ratios in the therapy couch surface were lower than 0.02%.
| Table 2 Leakage radiation dose distribution in the treatment couch plane of TOMO unit |
As the chief running characteristics of TOMO unit,a linear accelerator (6 MV X-rays) was mounted on the CT slip ring. The distance from the source to the center of rotation was 85 cm,and the typical fan beam field at isocenter was 40 cm×1 cm,40 cm×2.5 cm and 40 cm×5 cm,so the single therapy irradiation could be implemented up to 20 000 sub fields. The perfect uniformity and conformal degree of the target dose area could greatly improve the tumor treatment effect and prevent the side effects of treatment from the non-useful doses delivered to normal tissues. Moreover,the treatment range could be up to 160 cm through the continuous slow moving of couch in the whole body IMRT and it suitable for almost all cases which received TOMO radiation therapy. With more and more TOMO units being employed in clinical application because of the unique advantages over a conventional 6 MV linear accelerator,higher and higher level of quality control requirement was demanded for the equipment. A lot of specific and detailed testing items of quality control were given in AAPM technical report No.148,and a significant part of the index was same essentially,but there was no mature technology in our country at present. With the lack of independent technical methods for comparison,verification and validation outside of the manufacturer[7],the manufacturer's technicians should be monitored in the course of its own technology,equipment and testing methods being operated. The static and dynamic output dose,radiation quality,the stability of the horizontal/vertical dose distribution curve,the width of Jaw and leakage radiation ratios were selected as the core parameters of TOMO unit to reflect the status of QC and patient protection,and they were representative in the radiological protection work in tomotherapy.
The output dose errors under the conditions of static and dynamic state should be tested to judge whether the TOMO unit kept good stability and repeatability or not. Dynamic output dose measurement was a kind of comprehensive validation method to verify the performance of radiotherapy equipment,and almost all dynamic factors including gantry rotating,treatment couch movement,delay of multileaf collimator,lead Jaw width,synchronicity of multileaf collimator- gantry-couch on the output dose consistency can be assessed easily[8]. Quality control testing results at 221 d of the treatment equipment were reported by some scholars,and the statistical analysis showed that the deviation range of static output dosage was -3.8%-3.4%,the deviation of which 197 d (89.10%) of the data was in the range of -2.00%-2.00%,and no obvious law exists in the data distribution[9]. At the same time,the statistical analysis of the measurement results of dynamic output dose showed that the variation range was -1.50%-4.90%,and the data from 149 d (87.10%) was in the range of -2.00%-2.00% of the allowable deviation. In this study,the measurement result error of static output dose and dynamic output dose was -1.51% and 1.18%,respectively,all of them were less than 2.00% and in the allowable deviation range,but the stability of the dynamic output dose could be affected by the accelerated target aging and thinning which resulted from heavy workload of the equipment every day[10, 11]. In fact,the output dose was adjusted every 3 weeks according to the actual stability state of TOMO unit and some related research results provided by Broggi et al[8] in some hospital.
As a special image guided intensity-modulated radiation therapy equipment,TOMO develops inhomogeneous output dose without radiation flatness,which was different from the conventional accelerator in structure,and the other different dosimetric characteristics from the conventional accelerator resulted from small source-surface distance and high output dose rate. The analysis of percentage depth dose (PPD) and off-axis parameters showed that the maximum dose point was at the position of 1.5 cm from phantom surface for TOMO unit and conventional 6 MV accelerators,and there was no significant difference of these two radiotherapy units. In the research,PDD10 and PDD20 of TOMO unit were 61.00% and 31.90% respectively through on-site measuring,while the PDD10 and PDD20 were 66.80% and 39.20% respectively for 6 MV X-rays of ARTISTE accelerator,then the corresponding errors of PDD10 and PDD20 for the two radiotherapy units were 8.70% and 18.60%,respectively. Not only the existence of the differences between them had relationship with the structure characteristics,but also the other factors should be taken into account,such as the exposure conditions in measurement and the different scattered radiation environments with different test phantom. TOMO parameters were tested under the conditions of SSD 85 cm,and radiation field 40 cm×5 cm,while the ARTISTE accelerator under the conditions of SSD 100 cm and radiation field 10 cm×10 cm. Dose distribution inhomogeneity features of TOMO radiation field consist of cone-shaped dose distribution in human body at left-right direction (in the x direction) and obvious dose distribution fluctuation with the change of the beam width at head-foot direction (couch axis or the y direction). The accelerator radiation sources of TOMO unit had a certain size,the output dose contribution from adjacent multileaf collimator blades was larger than that of single leaf,and there was mutual influence on the absorbed dose between all adjacent leaves while opening and closing. It was reported that the output factors remained the same value even if the multileaf number increased continuously,and the radiation field output factors of multileaf collimator were all measured from tissue equivalent material of solid water under the condition of the number 32 leaf set with different irradiation range in this study.
Leakage radiation level of multileaf collimator and the unit itself is an important parameter of patient protection,as well as the practical reference of treatment room protection design because the core component of TOMO is accelerator. The leakage radiation ratio at rotation center from multileaf collimator of the TOMO unit was 0.20%,which was significantly lower than the specified value of 2.00% for conventional accelerator collimator radiation leakage ratio issued according to the National standard GBZ 126-2011[12]. Actually,the average leakage radiation ratio was usually between 0.11% and 0.40% through the collimator leakage of current clinical operation of conventional accelerators[13],and the leakage radiation of multileaf collimator of TOMO unit tested was equivalent to the value reported. Similarly,the leakage radiation levels at couch plane of TOMO were corresponding to the same parameter of conventional 6 MV accelerator treatment couch plane. The measurement range of leakage radiation was expanded because TOMO gantry was in the rotating state during test. Measurement results showed that the leakage radiation ratios of all directions in every point 1,2 and 3 m from rotation center were not higher than 0.02% on the treatment couch plane of TOMO,and less than 0.10% for average value and 0.20% for maximum value according to GBZ 126-2011,even far lower than the radiation leakage levels of conventional 6 MV accelerator,which was consistent with the results reported in the related literature[14].
In general,the performance and testing requirements of TOMO unit are different from conventional electron linear accelerator,the quality control index of TOMO unit should be set seperately,tested and analyzed periodically in terms of the specific requirements of the unit itself complying with the QC program strictly. The reliable quality control system should be established and effectively implemented to service for the radiotherapy quality and radiation safety effectively in the tomotherapy.
| [1] | Nguyen NP, Vock J, Sroka T, et al. Feasibility of image-guided radiotherapy based on tomotherapy for the treatment of locally advanced anal carcinoma[J]. Anticancer Res, 2011, 31(12): 4393-4396. |
| [2] | Balog J,Soisson E. Helical tomotherapy quality assurance[J]. Int J Radiat Oncol Biol Phys, 2008, 71 Suppl 1: S113-117. |
| [3] | Giraud P, Kantor G, Yassa M, et al. Two-year clinical experience with tomotherapy: the French National cancer institute project on implementing new technology[J]. Cancer Invest, 2011, 29(8): 557-563. |
| [4] | International Commission on Radiological Protection. ICRP publication 112. A report of preventing accidental exposures from new external beam radiation therapy technologies[J]. New York: Elsevier, 2009. |
| [5] | 吴伟章, 朱夫海, 王勇, 等. 旋转照射剂量测量仪(ArcCHECK)在螺旋断层放疗计划剂量验证中的应用[J]. 肿瘤预防与治疗,2014,27(1):20-23. |
| [6] | Langen KM, Papanikolaou N, Balog J, et al. QA for helical tomotherapy: report of the AAPM Task Group 148[J]. Med Phys, 2010, 37(9): 4817-4853. |
| [7] | 赵进沛,张富利,王雅棣,等. 热释光技术在螺旋断层放射治疗系统治疗计划剂量验证中的应用研究[J]. 中国职业医学,2014,41(1): 73-76. |
| [8] | Broggi S,Cattaneo GM,Molinelli S,et al.Results of a two-year quality control program for a helical tomotherapy unit[J].Radiother Oncol, 2008, 86(2): 231-241. |
| [9] | 管秋, 杨波,王欣海,等. TomoTherapy Hi-Art加速器剂量输出稳定性检测与评价[J]. 协和医学杂志, 2013, 4(4): 404-407. |
| [10] | Staton RJ, Langen KM, Kupelian PA,et al.Dosimetric effects of rotational output variation and X-ray target degradation on helical tomotherapy plans[J].Med Phys, 2009, 36(7): 2881-2888. |
| [11] | 徐寿平, 戴相昆, 解传滨, 等.螺旋断层放疗机束流输出稳定性测量及分析[J].中国医学物理学杂志,2009, 26(1): 945-948. |
| [12] | 中华人民共和国卫生部. GBZ 126-2011电子加速器放射治疗放射防护要求[S]. 北京:人民卫生出版社, 2011. |
| [13] | 马永忠, 娄云, 万玲,等. 36台医用加速器装置泄漏辐射水平测量与分析[J]. 中国职业医学,2011,38(3): 220-222. |
| [14] | 马永忠, 万玲, 娄云, 等. 螺旋断层放射治疗室内泄漏辐射与散射辐射监测与评价研究[J]. 中华放射医学与防护杂志, 2013, 33(4): 431-435. |